Featured in:
If you're reading this, then you probably believe all of the following things to be true:
In other words, you like to make decisions based on the best available evidence.
Yet, even with a scientific mindset, it can still be difficult to know what to do when you’re suffering from an episode of debilitating low back pain.
Do you visit your doctor who you know will only tell you to rest and take some pain pills (like he did last time)?
Do you go back to the osteopath who told you that you have the incorrigible condition of having one leg shorter than the other?
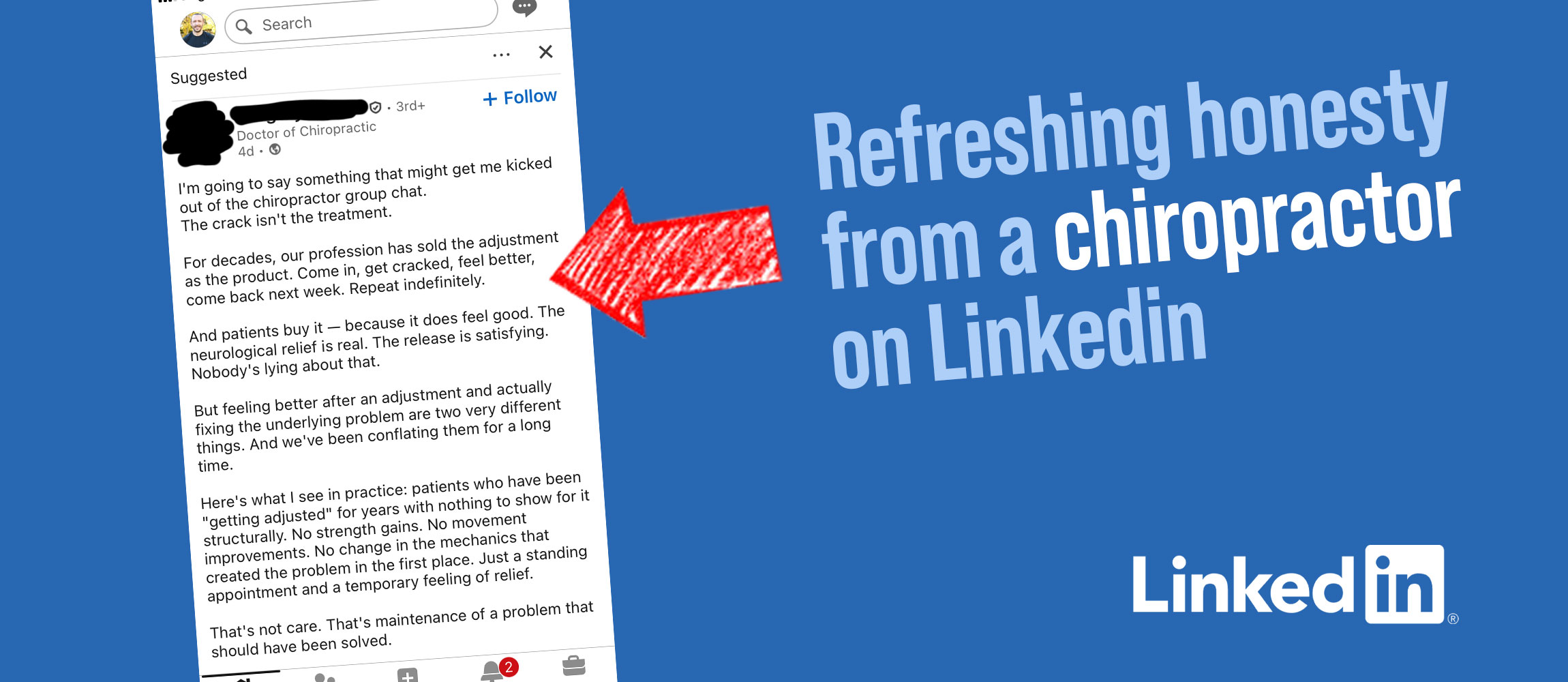
Or do you make an appointment with the chiropractor who violently twisted and cracked your neck without warning you (then invited you back for regular ‘adjustments’)?
I’m not saying that you shouldn’t see any of the professionals mentioned above because there are good and bad versions of all of them.
But, I have personally experienced each and every one of these encounters, exactly as described above. And, I know I’m not alone because I've heard similar stories from my clients.
To add to the confusion over the best course of action to take you may have read articles in the popular press claiming that ‘studies show’ that no treatment for non-specific low back pain is more effective than any other.
So, what should you do?
Fortunately, not all clinicians have conceded defeat. Professor Stuart McGill categorically states that 'there is no such thing as non-specific back pain. There are only poor diagnoses resulting from inadequate assessments.' He points out that low back pain is not a homogeneous condition like diabetes. It therefore requires non-homogeneous solutions. In other words, there are many different causes of back pain which means that its treatment needs to be adapted to the individual.
Generic treatments may help one individual but could just as easily harm another (as often happens when people with low back pain practice pilates or yoga). What each person actually needs is a thorough assessment and an individualised treatment plan.
Such an assessment would involve identifying the movements, postures and loads that cause pain in each person so they can learn how to avoid provoking their individual pain triggers. Their treatment plan can then be designed around these triggers.
The problem is that, by definition, an individualised treatment program can't be randomly assigned to different people. This inconvenient fact makes randomised controlled trials totally irrelevant in the study of a heterogeneous condition such as low back pain.
Nevertheless, many practitioners who claim to be 'evidence-based' continue to insist on this unrealistically high bar of evidence, routinely ignoring a mass of other evidence that provides a much more nuanced and plausible picture.
During a 32-year career as Professor of Spine Biomechanics at Waterloo University, Canada, Stuart McGill and his team of researchers amassed a body of work comprised of four pillars:
1. An in vitro lab
where, amongst other things, he investigated intervertebral disc injury mechanisms by conducting experiments on the cadaveric spines of humans and pigs (animal models were used in about 10% of studies because of the lack of availability of young, healthy, non-degenerated human specimens). Whilst ‘evidence-based’ critics were quick to point out that humans aren’t pigs (insert facepalm emoji here), they were slow to offer up human family members to replace the pigs in the experiments.
2. An in vivo lab
where he carried out studies on spinal stability by using motion sensor technology (similar to that used to create motion graphics films like Avatar). In doing so, he was able to create a virtual spine which enabled the measurement of loads and stresses on the various lumbar tissues.
3. A clinical practice
where he worked with a combination of elite athletes and patients with ‘failed backs’ who had been told their only option was surgery (McGill states that 95% of these individuals have successfully managed to avoid surgery after consulting with him).
4. Field testing
where studies were carried out on physically active populations including the police, firefighters, the military, sports teams and occupational groups.
‘From the perspective of injury mechanics and exercise prescription, the flexion issue is complex. The approach should not be guided by a single study, not one on pigs, humans, or within institutions such as the military. But all together, all of these studies are important.’
The most well-known, and poorly understood of McGill’s experiments are those involving pig spines. They showed that subjecting the porcine spines to repeated flexion under compressive load is an effective injury-mechanism to healthy spines, often resulting in herniation of the intervertebral discs. This has important implications for lifting techniques employed by humans who want to avoid injuring their backs.

However, critics interpreted this to mean that you should never flex the spine, whilst pointing to examples of athletes who routinely do. This quote from McGill's response to his critics, provides a more accurate summary of what he actually says on the matter:
'If the spine is under load, it is best not to move it—that is, to keep it stiff. This principle is not contestable. However, if the spine must flex such as when a strongman event competitor lifts an atlas stone, it should be held in an isometrically flexed posture.... The spine does not move because the motion is focused about the hip joints until the final 'hoik'... The worst technique would be to move the spine into flexion, over and over, so the combination of load with motion would slowly and cumulatively delaminate the disc collagen.'

McGill goes on to say: 'From the perspective of injury mechanics and exercise prescription, the flexion issue is complex. The approach should not be guided by a single study, not one on pigs, humans, or within institutions such as the military. But all together, all of these studies are important.'
Yet, despite this nuanced approach that takes into account multiple sources of evidence, many of the 'evidence-based' crowd conclude that most of these studies are unimportant because they don't meet the gold standard of randomised controlled trials.
As a result, bio-mechanical explanations of low back pain have been shunned in favour of vague psycho-social explanations: 'the pain is in your head'. Or defeatist declarations that pain is complicated: 'we don't really know what causes it'.
Unfortunately, this can lead sufferers of low back pain to feel disempowered and develop a fear of movement because they're unaware of how to avoid triggering their pain. Even worse, they can end up re-injuring their backs by persisting with the same faulty movement mechanics that got them injured in the first place.
Hence the confusion about the best course of action to take when you've got a bad back.
However, I recently came across a striking parallel in another field which shows that this muddled thinking isn't limited to the world of low back pain.
Trisha Greenhalgh has been one of my go-to references for information on COVID-19 since the start of the pandemic. She's the Professor of Primary Care Health Sciences at Oxford University and recently gave a lecture online about how social science can help us survive the post-truth pandemic.
Whilst watching the video above I couldn't help but draw parallels between deniers of the efficacy of masks (against the spread of SARS-CoV-2) and critics of The McGill Method, the methodology developed by Professor Stuart McGill, which, as previously described, takes a more nuanced approach to the treatment of low back pain.
Greenhalgh explains the existence of distinct intellectual tribes in academia, pointing out important differences in the way they interpret evidence.
First up is the Evidence-Based Medicine (EBM) tribe. Their totem is 'the hierarchy of evidence', atop which sit 'systematic reviews and randomised controlled trials'. All other forms of evidence are seen as being inferior to this.
Then there's what she refers to as the Pragmatic Public Health (PPH) tribe (which Greenhalgh identifies herself with). Their totem is 'the real world case study'. Tribe members strongly believe that 'there is no universally applicable hierarchy of evidence, although some methods may be more fit for purpose.'
These two tribes, while both well-intentioned, had very different views regarding the efficacy of masks at the beginning of the COVID-19 pandemic.
Two members of the EBM tribe, Jefferson and Henegan, conducted a systematic review of all the evidence deemed valid by their tribe: they identified all randomised controlled trials that looked at the efficacy of masks in preventing respiratory infections.
They chose not to look at other types of research because these had already been classified as inferior by their tribal rules. As Greenhalgh explains, 'they placed all non-randomised controlled trials in a metaphorical trash can'.
As a result of these questionable assumptions, they only had randomised controlled trials to guide them. So, while a lethal pandemic was ripping through the world, they concluded that there was no good evidence for the efficacy of masks.
Hmmm, does this reasoning sound familiar?
‘One year and 3 million deaths later, the EBM tribe were still arguing over whether SARS-CoV-2 was airborne.’
However, Greenhalgh and her PPH tribe took a very different approach. They believe that 'good science is defined by the use of multiple methods, adaptively and pragmatically, to build a nuanced narrative of what has happened and why.' She states that 'theory is at least as important as method,' and that 'the narrative needs to make sense and be plausible to the natives'.
This allowed additional evidence to be brought to the table (studies that had been ignored by the EBM tribe):
1) Videos where people sneeze, emitting huge clouds of airborne particles
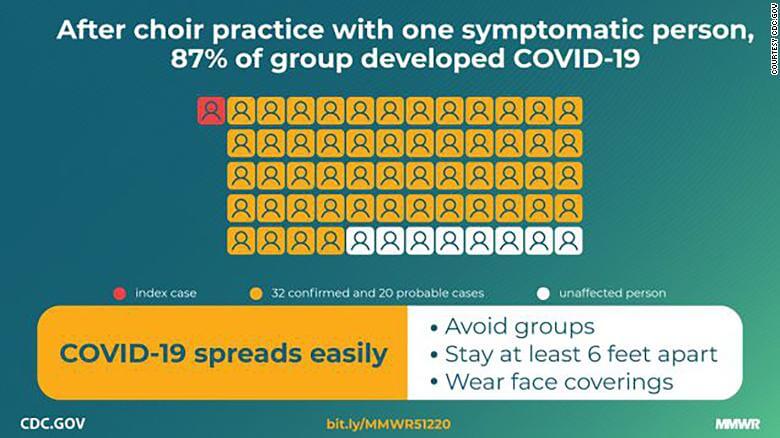
2) Choir practices where people became infected even when they didn't get within 6 feet of the index case or touch common surfaces.
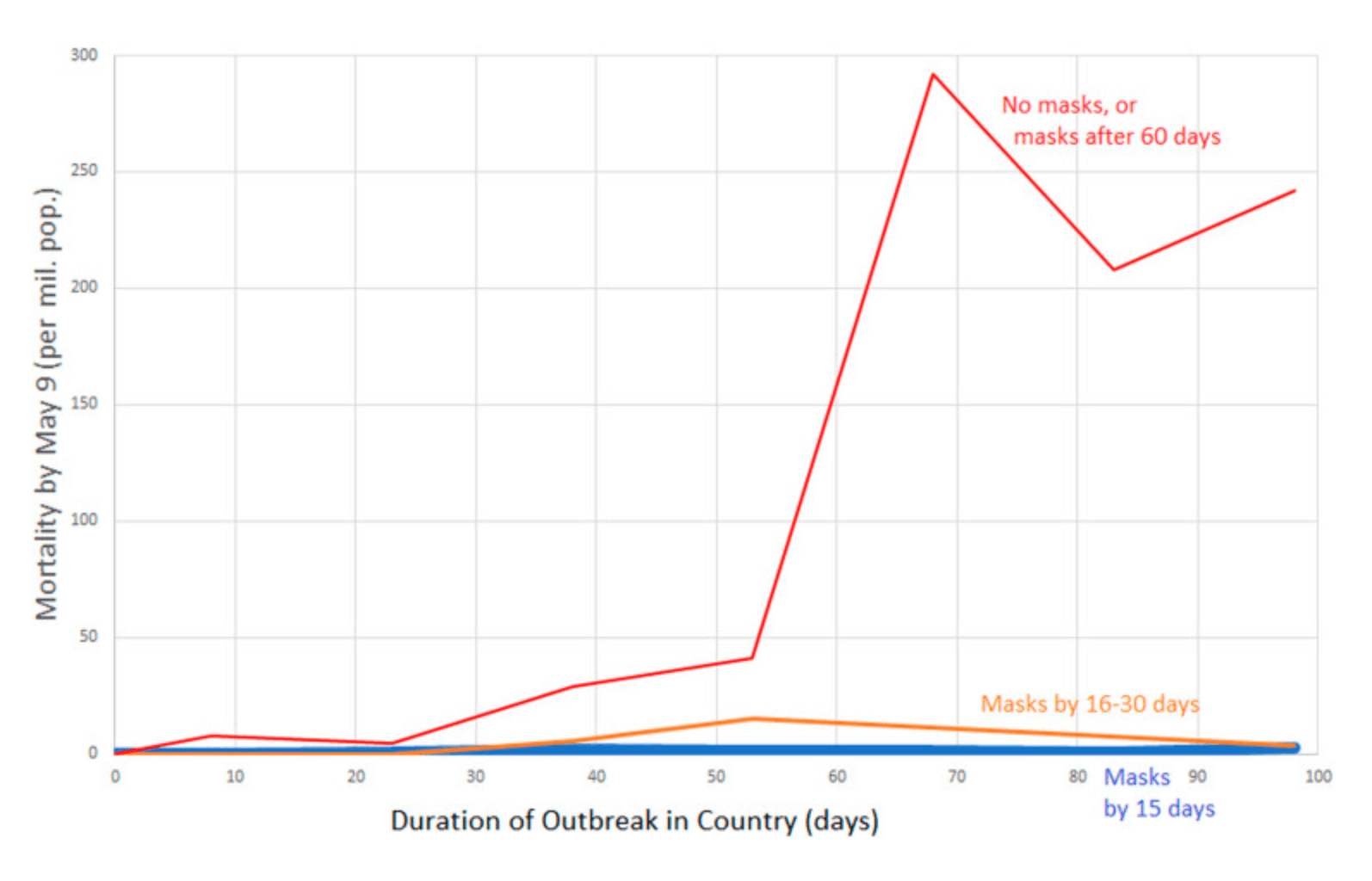
3) Natural experiments around the world: where there were orders of magnitude fewer deaths in countries where masks were mandated.
She points out that these pieces of evidence taken in isolation are not proof that masks work. However, they do add to the overall picture and demand a scientific explanation.
She and her colleagues wrote an article that was published in the BMJ in which they argued for the precautionary principle. They stated that while there is no proof that masks work 100% yet, we should still act pragmatically on the basis of numerous facts that point in the direction of the positive benefit of mask-wearing.
That was back in March 2020. One year and 3 million deaths later, the EBM tribe were still arguing over whether SARS-CoV-2 was airborne.
Much the same confusion still persists in the world of low back pain, with similarly dire (though, usually not fatal) results.
A wealth of evidence from studies involving in vitro and in vivo experiments, to studies of elite athletes and active populations provides a nuanced narrative of the causes of low back pain, how to treat it on an individual level and how to avoid injuring your back in the first place.
Yet, much of this biomechanical evidence is often ignored because it doesn't meet the unrealistic criteria determined by the beliefs of the EBM tribe.
This leads to 'evidence-based' practitioners telling their patients and social media followers that it's ok to deadlift with a fully flexed lumbar spine... that how you move isn't important, as long as you move... that it doesn't matter how you sit, etc, etc... All the while, proudly declaring their certainty because there aren't any randomised control trials that show the contrary.
I believe that this results in a lot of people suffering from low back pain that’s entirely avoidable.
The good news is that if you understand the value of evidence provided by pig spines and mask mandates, not only will you have a better chance of avoiding Covid, but you'll also have a better idea of how to get rid of your back pain.